When Golisano Children’s Hospital at UK integrated a child life specialist into its perioperative team, leaders expected improvements in the patient experience.
What they didn’t anticipate was a major shift in clinical practice.
Within months, the hospital saw a nearly 50% reduction in pre-procedure sedation for children undergoing surgery.
The team didn’t set out to reduce sedation. Instead, the results emerged naturally after changing how they addressed kids’ anxiety in operating rooms.
“When the anxiety in the room goes down, anesthesia assessments change,” said Jennifer Guilliams, director of child life services. “Sometimes the team realizes they don’t need the medication.”
The effect of child life education
Golisano Children’s operates within the broader UK HealthCare system, where operating rooms serve both adult and pediatric patients.
That structure meant children were often moving through environments and workflows designed primarily for adult patients.
“For hospitals embedded in adult systems, this is often the challenge,” Guilliams said. “You’re providing pediatric care in spaces that weren’t designed for kids. But you can still change how that care feels.”
In 2023, the hospital added one full-time certified child life specialist dedicated to perioperative services to strengthen pediatric support across the surgical journey.
One of the first priorities was education.
“The biggest return was empowering staff,” Guilliams said. “Once people felt like they had something they could do, everything changed.”
The child life specialist trained nurses, surgeons, anesthesiologists, and operating room technicians in several areas:
- How anxiety presents across developmental stages
- Language choices that reduce distress
- Strategies to support coping during IV placement and anesthesia induction
- Techniques to maintain a child’s sense of control
The goal was not to replace clinical workflows but to strengthen them with pediatric-specific expertise.
“We just needed to shift some of the ways we approached children so interactions were more pediatric-focused,” Guilliams said.
That education extended into daily practice. The child life specialist paired with staff during cases, modeling language, demonstrating distraction techniques, and helping teams interpret behavioral cues in real time.
"For hospitals embedded in adult systems, this is often the challenge. You’re providing pediatric care in spaces that weren’t designed for kids. But you can still change how that care feels."
Over time, those practices began to influence how the team approached anxious patients — often reducing the need for pharmacologic intervention.
“These were small changes,” Guilliams said. “But together, they changed how kids experienced the entire process.”
Child life at the bedside
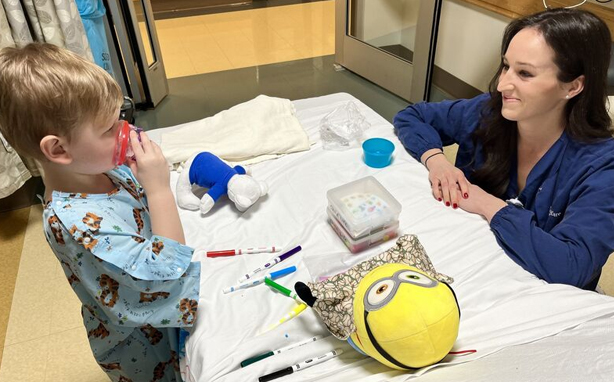
Alongside staff education, the child life specialist remained embedded in daily clinical care.
She used medical play to help kids get comfortable with wearing anesthesia masks, provided comfort tools during IV placements, and accompanied patients through the surgery, providing continuity as they were separated from their caregivers.
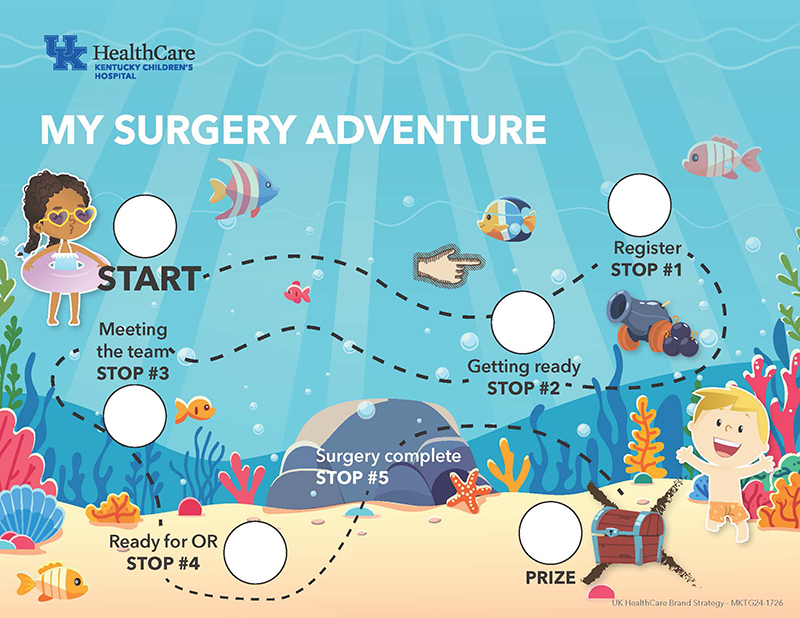
She introduced a “treasure map” that guided children step‑by‑step through the surgical day, helping them understand what was coming and when it would end. When the child completed their task, like getting their gown on or walking to the OR, they got a sticker to mark the spot. At the end, during recovery, they received their “treasure” — a coin they could use in a prize machine.
“Even though this was developed by child life, it was really important that it be staff-driven,” Guilliams said. “We wanted everybody to have something they could contribute to make the experience more kid friendly.”
These supports helped reduce uncertainty and give children a sense of predictability during a stressful experience.
Early outcomes
During the initiative’s first year, the team made 1,246 child life interventions, reaching more than 40% of pediatric patients who underwent surgery.
Families felt the impact. Feedback frequently highlighted the calming presence of child life staff and the role they played in helping children feel prepared for surgery.
The initiative also strengthened interdisciplinary collaboration. Even after the original child life specialist left the role, the practices she established continued. Nursing teams maintained the tools, and anesthesia teams advocated for child life involvement.
“This wasn’t about one person doing distraction,” Guilliams said. “It was about teams having better tools, shared language, and better assessments.”
Based on the early results, surgical leadership approved funding to add another child life specialist to expand support across additional surgical areas.
Future plans include pre-surgical screening calls and the development of child-friendly educational tools to help families prepare for procedures.
“We know we can’t have a dedicated child life specialist everywhere,” Guilliams said, “but when you give staff new tools and ways to interact with kids, it can change everything.”


